
In my previous post (see The Clinic Door – Chapter 1: The Beginning) I mentioned becoming ill in August and my introduction to the healthcare system from the perspective of consumer rather than provider.
About a month down from the road from that post, I have had other experiences I hope to talk about but the emergency room (ER) perhaps was one of my favorite experiences to date.
 I had been driving and developed increasingly worse “heavy” chest pain and could not breath with marked sweating. I turned into the nearest hospital parking lot and backed in the car to a spot close to the ER door. The waiting room was relatively empty on this weekday morning and the reception desk was open. I told the admitting clerk “I have chest pain and shortness of breath”. Those apparently are key words ER clerks are taught to make things happen. Within a few minutes, I was whisked back to a room, sitting on a gurney, on an EKG monitor, given oxygen, IV access and had labs drawn. A couple of nurses took some additional medical history and asked about drug allergies, family history and acuteness/chronicity of my symptoms.
I had been driving and developed increasingly worse “heavy” chest pain and could not breath with marked sweating. I turned into the nearest hospital parking lot and backed in the car to a spot close to the ER door. The waiting room was relatively empty on this weekday morning and the reception desk was open. I told the admitting clerk “I have chest pain and shortness of breath”. Those apparently are key words ER clerks are taught to make things happen. Within a few minutes, I was whisked back to a room, sitting on a gurney, on an EKG monitor, given oxygen, IV access and had labs drawn. A couple of nurses took some additional medical history and asked about drug allergies, family history and acuteness/chronicity of my symptoms.
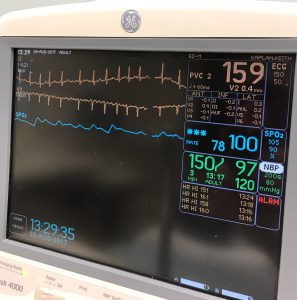 A few minutes later the ER physician introduced herself, asked how I was feeling, saw I looked like I belonged there and told me I was in atrial fibrillation with a heart rate of 170.
A few minutes later the ER physician introduced herself, asked how I was feeling, saw I looked like I belonged there and told me I was in atrial fibrillation with a heart rate of 170.
Atrial fibrillation? Heart rate of 170? Are you kidding me? What’s causing this?
Between the labs and history many causes/associations were excluded, some medications were given for heart rate control and was told “I bought a bed for the night”.
And I could be cardioverted in the ER to try to see if I could get into a normal sinus rhythm.
Cardioverted? What’s that?
It has been a few years (nearly 25) since my cardiology rotation during the Summer in Chicago where my goal was to get out early and ride my bike along the lake rather than master cardiac physiology and therapeutics.
I was advised blood thinners would be started, some oral and IV medication would be given for rate control, she would do a transesophageal echocardiogram (TEE) to look for any blood clots, if there weren’t any, paddles would be applied to my chest and back after I was sedated and some electricity would be applied to the pads. A crash cart would be on hand. Anesthesia would be called.
Electricity? How much electricity? Anesthesia? We just met. Shouldn’t we get to know me a little better first?
Your heart is running a marathon and likely has stretched out your heart including your left atrium and causing this abnormal rhythm.
I am laying here hardly running anywhere. Are you sure about this? Can I phone a friend? Blood thinners? A tube down my throat and electricity across my chest?
The ER physician told me her shift ends in 15 minutes and to let her know what I wanted to do.
How about sign out of this place AMA before your shift ends?
This is one observation I have made across multiple healthcare organizations as a consumer getting hospitalized (and re-hospitalized) and being seen by multiple providers. Clinicians are increasingly working on shifts. The ER of course has always worked this way with physicians doing their 12-hour shifts several days (or nights) a week to provide a physician in the room.
And once you get handed off from one ER physician to the next, a hospitalist, until about 7 PM takes over until the 7 PM – 7 AM hospitalist comes in and gets you through the day until the 7 AM – 7 PM hospitalist comes back.
But also, the office hours are very tightly controlled by healthcare systems, with certain providers at certain locations certain days of the week and no ands, ifs or buts if you want to go to one location and your physician isn’t hanging up their shingle that day or afternoon.
When the specimen container comes into the lab and the slides appear the next day, this was lost on me a bit. Sure, Dr. So and So operates Tuesdays and Thursdays and every other Wednesday but I assumed he/she was in “clinic” in one location the other days. It could be 3 or 4 other “clinics”. Of course, pathologists may cover more than 1 hospital as well but I have found some periodicity to this in the past 20 years. You might go to hospital X every month for 1 week and cover hospital Y every Friday. Clinicians, in my experience, trying to schedule appointments and chase them around to 4 different offices, do not have the same periodicity.
One significant reason for this is physicians may be part of more than one “system”. They may be affiliated with Company A and Company B and Company C. The same group of cardiologists may have 3 different white coats with 3 different logos, depending on where they are in a morning or afternoon (forget about evening appointments after work).
A consumer needs to be a little careful here as your visit notes and labs and tests will likely end up in a different database than your “primary” database. Another patient portal with different information and no connection to the other databases or portals. Even if the different hospitals have the same EMR vendor…So much for interoperability. It is just as frustrating as a consumer as it is for a provider.
More in Part 3 on being hospitalized and subsequent follow up within the healthcare system.














